Common Names
- Vinpocetine
- Periwinkle
- Vinca minor
- Kavinton; Cavinton
- Rgh-4405
- Tcv-3B
- Apovincaminic acid
For Patients & Caregivers
Tell your healthcare providers about any dietary supplements you’re taking, such as herbs, vitamins, minerals, and natural or home remedies. This will help them manage your care and keep you safe.
Vinpocetine may be useful against some cerebrovascular disorders, but additional studies are needed.
Vinpocetine is made from a compound found in the common periwinkle plant. It was developed in Europe as a drug but is sold in the United States as a dietary supplement to improve brain function.
Vinpocetine may increase blood flow to the brain and has been studied as a treatment for Alzheimer's disease and for disorders of the nervous and circulatory systems. However, more studies are needed before it can be recommended.
Vinpocetine should not be confused with the chemotherapy drugs vincristine and vinblastine, which are also made from compounds of the periwinkle plant.
- Alzheimer's disease
Small studies suggest benefit, but well-designed clinical trials are needed. - Cognitive decline
Vinpocetine may improve cognitive decline, but more studies are needed. - Dementia
A systematic review did not find benefit with vinpocetine for dementia. - Memory loss
A few clinical trials have shown benefit. Large-scale studies are needed. - Stroke
Some studies suggest benefits in stroke patients, but larger studies are needed. - Cancer treatment
Lab studies suggest some anticancer and increased radiation effects on tumor cells, but this has not been studied in humans.
- Flushing, rashes, gastrointestinal problems
- Low blood pressure
- Decreased white blood cell count
In a small study, jitters, increased heart rate, and insomnia were possibly related.
Case reports
- Skin reaction, rapid heartbeat, stomach ache: In a man who took a supplement containing Ginkgo biloba and vinpocetine. However, it is uncertain whether both ingredients contributed equally to these reactions.
- Low white blood cell counts: In a 73-year-old man after using vinpocetine for 50 days. His symptoms resolved after product discontinuation.
Patient Warnings:
- A report from the National Toxicology Program of the National Institutes of Health suggests this supplement may cause harm to pregnant women or the fetus. In supplement labeling, vinpocetine may also be called periwinkle or vinca minor extract.
- Patients with low blood pressure, a history of heart problems or strokes, or those on cardiovascular medications should consult their physician before using this product.
Do Not Take if:
- You are pregnant: A report from the National Toxicology Program of the National Institutes of Health suggests this supplement may cause harm to pregnant women or the fetus. In supplement labeling, vinpocetine may also be called periwinkle or vinca minor extract.
- You are using blood-thinning drugs: Vinpocetine may increase their effects.
- You are taking medication to lower high blood pressure: Vinpocetine may enhance their effects.
- You are taking P-glycoprotein substrate drugs: Lab studies suggest that vinpocetine may alter the way these drugs work in the body. Clinical relevance is not yet known.
For Healthcare Professionals
Vinpocetine is derived from vincamine, an alkaloid found in the common periwinkle plant. Originally developed in Europe where it is marketed as a drug called Cavinton, vinpocetine is sold in the United States as a dietary supplement to improve brain function.
Animal models suggest that vinpocetine has anti-inflammatory, antioxidant, antimitotic, antiatherogenic, antithrombotic, and antiepileptic effects (1) (2) (3) (4) (5) (6) (7).
Human studies suggest vinpocetine enhances short-term memory (8), cognitive performance (9), and improves chronic cerebral dysfunction in elderly patients (10). It has also been studied as a potential treatment for Alzheimer’s disease (11), but a systematic review did not find benefit (12). In both healthy adult volunteers and patients with focal epilepsy, no significant cognitive benefits were seen with the vinpocetine dosages tested (33).
Other small studies suggest vinpocetine may help maintain or improve hemorheologic parameters in patients with cerebrovascular disorders (13) (28), but a systematic review did not find enough evidence for benefit in patients with acute ischemic stroke (14). In a randomized open-label study, intravenous vinpocetine adjunctive to treatment for acute cerebral infarction improved cerebral blood flow, neurological functioning, and cognition (29).
Vinpocetine inhibits the growth of breast cancer cells in vitro and in vivo (15). In animal studies, it potentiates the effects of radiation therapy in tumor cells (16). In nasopharyngeal carcinoma patients following radiation injury, preliminary data suggest potential with a combination of vinpocetine and dexamethasone for cognitive impairment compared with dexamethasone alone (34). However, studies in cancer patients in general are lacking.
Vinpocetine should not be confused with chemotherapy drugs such as vincristine or vinblastine, which are also alkaloids derived from the periwinkle plant.
- Alzheimer’s disease
- Cognition
- Dementia
- Memory loss
- Stroke
- Cancer
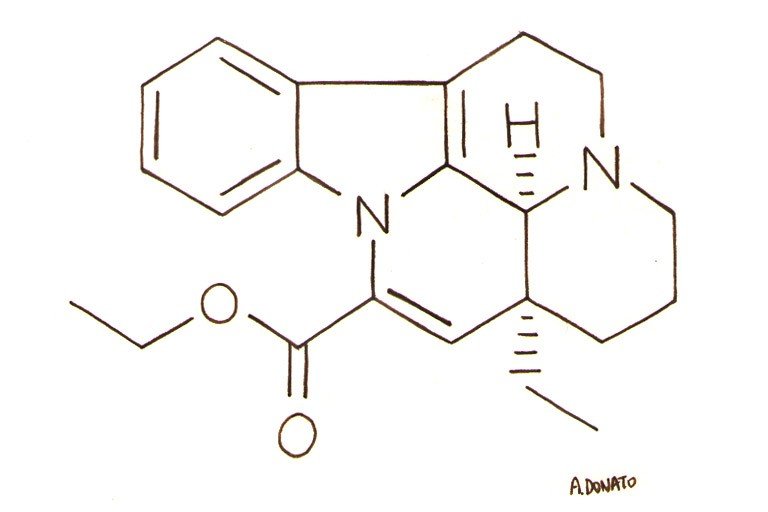
Vinpocetine is a synthetic ethyl ester of apovincamine derived from an alkaloid in the common periwinkle plant (17). In vitro, antioxidant and hydroxyl radical scavenging properties have been observed (18) (13). Vinpocetine inhibits PDE1 activity and improves cerebral blood flow by elevating cGMP and cAMP, increasing mitochondrial function, and improving glucose and oxygen utilization by the brain. Vinpocetine helps improve spatial memory in rats by preventing neuronal damage and favorably modulating cholinergic function (18). Antiepileptic effects were attributed to suppression of abnormal neuronal excitability via sodium channel regulation and dopamine release in striatal nerve endings (5) (6) (7). Vinpocetine antagonizes platelet-derived growth factor-induced extracellular matrix synthesis, suppresses intracellular ROS production, and inhibits extracellular signal-regulated kinase 1/2 activation and vascular smooth muscle cell growth (4). Antiatherogenic effects occur through inhibition of monocyte adhesion, oxidative stress, and inflammatory responses mediated by protein kinase B/nuclear factor kappa B-dependent pathways (3). Vinpocetine also demonstrates anti-inflammatory effects by inhibiting TNF-α-induced NF-κB activities (19) as well as Akt and STAT3 activation (15). In a murine model of otitis media, vinpocetine suppressed S. pneumoniae-induced mucus production through mucin MUC5AC inhibition (27).
In vitro and in vivo studies indicate vinpocetine antitumor activity against human breast cancer cells occurs through G0/G1-phase cell cycle arrest and mitochondrial pathways of apoptosis (15). Vinpocetine may also increase the effects of radiation by increasing tumor oxygenation (16).
In humans, administration of vinpocetine to chronic stroke patients increased glucose uptake and release in unaffected areas of the brain (12). In a study of adjuvant vinpocetine, nasopharyngeal carcinoma patients had lower levels of serum inflammatory cytokines compared to those who received dexamethasone monotherapy (34).
A report from the National Toxicology Program of the National Institutes of Health suggests this supplement may cause harm to pregnant women or the fetus (30). In supplement labeling, vinpocetine may also be called periwinkle or vinca minor extract.
Patients with low blood pressure, a history of heart problems or strokes, or those on blood-thinning medications should consult their physician before using this product.
Rare: Flushing, rashes, gastrointestinal problems (23), hypotension (24)
In a small study, jitters, increased heart rate, and insomnia were possibly related (33).
Case Reports
Fixed drug eruption, tachycardia, gastrointestinal pain: In a man who ingested a natural product containing Ginkgo biloba and vinpocetine (31). However, it is uncertain whether both ingredients contributed equally to these reactions.
Agranulocytosis: In a 73-year-old man after using vinpocetine for 50 days. His symptoms resolved after discontinuing vinpocetine (25).
- Anticoagulants/antiplatelet agents: Vinpocetine may have additive effects and can increase risk of bleeding (13) (14) (26).
- Antihypertensive agents: Vinpocetine may increase hypotensive effects (24).
- P-glycoprotein substrates: In vitro studies indicate that vinpocetine strongly inhibits P-gp and may therefore alter the pharmacokinetics of substrate drugs (32). Clinical relevance has yet to be determined.