This information will help you get ready for your prostate artery embolization (EM-boh-lih-ZAY-shun). It will also help you understand what to expect after your procedure.
About your prostate
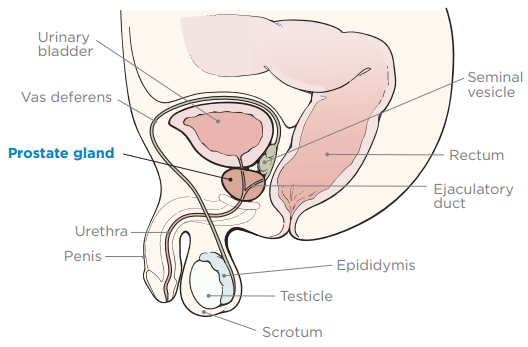
- Your prostate is a small, firm gland about the size of a walnut. It’s in front of your rectum, below your bladder (see Figure 1). Your prostate works with other glands in your body to make semen.
- Your urethra (yoo-REE-thruh) is a tube that carries urine (pee) from your bladder, through your penis, and out of your body.
- Your seminal vesicles are small glands near your prostate that make the fluid in semen.
What is a prostate artery embolization?
A prostate artery embolization is a procedure to block the arteries (blood vessels) in your prostate. It’s a treatment for benign prostatic hyperplasia (beh-NINE prah-STA-tik HY-per-PLAY-zhuh), also called BPH. Benign means it’s not cancer. BPH is when your prostate becomes enlarged (bigger than normal). Blocking the arteries in your prostate stops the blood flow to your prostate. This makes your prostate shrink.
About BPH
When you have BPH, your enlarged prostate presses down on your urethra. This can change the way you urinate (pee).
BPH is common in men over the age of 40. It can get worse as you age. BPH happens in:
- 4 out of every 10 men over the age of 40.
- 5 out of every 10 men over the age of 50.
- 6 out of every 10 men over the age of 60.
With BPH, you may feel like you need to urinate often. After you urinate, you may feel like your bladder isn’t empty.
The most common symptoms of BPH are:
- Frequent urination. This is when you urinate often, such as every 2 hours or less.
- Urinary urgency. This is an urgent need to urinate. You feel like you must urinate right away, or you may have an accident.
- Nocturia (nok-TER-ree-uh). This is when you wake up to urinate many times during the night.
- Urinary hesitancy. This is when you have a hard time urinating. You may have trouble starting or have a weak urine stream or dribbling.
- Intermittency. This is when you feel like you emptied your bladder but then need to urinate again a few minutes later.
- Acute urinary obstruction. This is when you’re not able to empty your bladder at all, or you have pain when urinating.
If you do not empty your bladder for long periods of time, you may get:
- A urinary tract infection (UTI).
- Bladder stones.
- Bladder diverticulum (DY-ver-TIH-kyoo-lum). This is when your bladder wall stretches and creates pockets that collect urine.
- Kidney damage from urine that backs up into your kidneys. This happens when your urethra is blocked.
About your prostate artery embolization
An interventional radiologist (also called an IR doctor) will do your prostate artery embolization. IR doctors have special training in using image-guided procedures. They use pictures from X-rays, magnetic resonance imaging (MRI) scans, computed tomography (CT) scans, or ultrasounds to help them.
You’ll meet with the IR doctor who will do your prostate artery embolization. They’ll explain the procedure to you and answer your questions. You’ll be asked to sign a consent form, which says you agree to the procedure and understand the risks. Your IR doctor will thread a catheter into the small arteries of your prostate. They’ll use X-rays to guide the catheter to the right place. Then, they’ll inject (put) very small particles through the catheter into your arteries. The particles will block the blood flow to your prostate and make it shrink.
The prostate will begin to shrink right away. It will take about 2 weeks to 3 months to see changes in you symptoms.
Your procedure will be done with a local anesthetic (medicine that numbs an area of your body). You’ll also get intravenous (IV) pain and sedation (seh-DAY-shun) medicine that will keep you comfortable during the procedure.
You’ll go home the same day as your procedure.
What to do before your prostate artery embolization
Ask about your medicines
You may need to stop taking some of your usual medicines before your procedure. Or, you may need to take a different dose (amount) than usual. Talk with your healthcare provider about how to take your medicines before your procedure. Do not change how you take your medicines without talking with a healthcare provider.
This section lists some examples of medicines, but there are many others. Make sure your care team knows all the prescription medicines, over-the-counter medicines, and dietary supplements you take. A prescription medicine is one you can only get with a prescription from a healthcare provider. An over-the-counter medicine is one you can buy without a prescription.
It’s very important to take your medicines and supplements the right way in the days before your procedure. If you don’t, we may need to reschedule your procedure.
Anticoagulants (blood thinners)
A blood thinner is a medicine that changes how your blood clots. Blood thinners are often prescribed to help prevent a heart attack, stroke, or other problems caused by blood clots.
If you take a blood thinner, ask your healthcare provider what to do before your procedure. They may tell you to stop taking it a certain number of days before your procedure. This will depend on the type of procedure you’re having and the reason you’re taking a blood thinner.
Here are some examples of blood thinners. There are others, so be sure your care team knows all the medicines you take. Do not stop taking your blood thinner without talking with a member of your care team.
|
|
Other medicines and supplements can change how your blood clots. Examples include vitamin E, fish oil, and nonsteroidal anti-inflammatory drugs (NSAIDs). Read How To Check if a Medicine or Supplement Has Aspirin, Other NSAIDs, Vitamin E, or Fish Oil. It will help you know which medicines and supplements you may need to avoid before your procedure.
Diabetes medicines
You may be taking insulin or other diabetes medicines. If so, talk with your MSK healthcare provider and the healthcare provider who prescribes it. Ask them what to do before your surgery or procedure. You may need to stop taking the medicine or take a different dose (amount) than usual. You may also need to follow different eating and drinking instructions before your surgery or procedure. Follow your healthcare provider’s instructions.
Your care team will check your blood sugar levels during your surgery or procedure.
GLP-1 medicines for weight loss
You may be taking a GLP-1 medicine. If so, it’s important to tell your healthcare provider. You will need to follow special eating and drinking instructions before your surgery or procedure. It is very important to follow these instructions. If you do not follow them, your surgery or procedure may be delayed or canceled.
- Follow a clear liquid diet the day before your surgery or procedure. Do not eat any solid food. Read Clear Liquid Diet to learn more.
- Stop drinking 8 hours before your arrival time. Do not eat or drink anything after this time, including clear liquids. You can have small sips of water with your medicines.
To learn more, read Eating and Drinking Before Your Surgery or Procedure When Taking GLP-1 Medicines.
Here are some examples of GLP-1 medicines. There are others, so be sure your care team knows all the medicines you take. Sometimes, these are prescribed to help manage diabetes or other conditions. Other times, they’re prescribed for weight loss.
|
|
Diuretics (water pills)
A diuretic is a medicine that helps control fluid buildup in your body. Diuretics are often prescribed to help treat hypertension (high blood pressure) or edema (swelling). They can also be prescribed to help treat certain heart or kidney problems.
You may be taking a diuretic. If so, ask the healthcare provider doing your procedure what to do before your procedure. You may need to stop taking it the day of your procedure.
Here are some examples of diuretics. There are others, so be sure your care team knows all the medicines you take.
|
|
Take devices off your skin
You may wear certain devices on your skin. Before your procedure, surgery, or scan, some device makers recommend you take off your:
- Continuous glucose monitor (CGM)
- Insulin pump
Talk with your healthcare provider about scheduling your appointment closer to the date you need to change your device. Make sure to bring an extra device with you to put on after your procedure, surgery, or scan.
You may not be sure how to manage your glucose (blood sugar) while your device is off. If so, before your appointment, talk with the healthcare provider who manages your diabetes care.
Stop taking nonsteroidal anti-inflammatory drugs (NSAIDs)
NSAIDs, such as ibuprofen (Advil® and Motrin®) and naproxen (Aleve®), can cause bleeding. Stop taking them 2 days before your procedure. If your healthcare provider gives you other instructions, follow those instead.
To learn more, read How To Check if a Medicine or Supplement Has Aspirin, Other NSAIDs, Vitamin E, or Fish Oil.
Reactions to contrast dye
Contrast is a special dye that makes it easier for your IR doctor to see differences in your internal organs. Internal organs are the organs inside of your body. This procedure is most often done with contrast.
Some people can have an allergic reaction to contrast. Most reactions are mild, such as hives.
Some people can have very rare but more serious reactions, such as anaphylaxis (A-nuh-fih-LAK-sis). This is a very bad allergic reaction that can cause hypotension (a sudden drop in blood pressure) or trouble breathing.
Anaphylaxis is treated with an epinephrine (eh-pih-NEH-frin) autoinjector, commonly known as an EpiPen®. This is an injection (shot) of epinephrine (adrenaline) into a muscle.
Tell your healthcare provider if you have had an allergic reaction to contrast dye in the past. You may need to take medicine before your procedure to help with the allergy.
Arrange for someone to take you home
You must have a responsible care partner take you home after your procedure. A responsible care partner is someone who can help you get home safely. They should be able to contact your care team if they have any concerns. Make sure to plan this before the day of your procedure.
If you don’t have a responsible care partner to take you home, call one of the agencies below. They’ll send someone to go home with you. There’s a charge for this service, and you’ll need to provide transportation. It’s OK to use a taxi or car service, but you still need a responsible care partner with you.
| Agencies in New York | Agencies in New Jersey |
| VNS Health: 888-735-8913 | Caring People: 877-227-4649 |
| Caring People: 877-227-4649 |
Note the time of your appointment
A staff member will call you 1 to 2 business days before your procedure. If your procedure is scheduled for a Monday, they’ll call you on the Thursday or Friday before. They’ll tell you what time to get to the hospital for your procedure. They will also remind you where to go.
If you don’t get a call by noon (12 p.m.) on the business day before your procedure, call 646-677-7001. If you need to cancel your procedure for any reason, call the healthcare provider who scheduled it for you.
What to do the day before your prostate artery embolization
Instructions for eating
Stop eating at midnight (12 a.m.) the night before your surgery or procedure. This includes hard candy and gum.
Your healthcare provider may have given you different instructions for when to stop eating. If so, follow their instructions. Some people need to fast (not eat) for longer before their surgery or procedure.
Medicine to prevent reaction to contrast dye
Your doctor may have told you to take medicine to prevent an allergic reaction to contrast. If they did, take the first dose 13 hours before your arrival time. Take the second dose 2 hours before your arrival time.
What to do the day of your prostate artery embolization
Instructions for drinking
Between midnight (12 a.m.) and 2 hours before your arrival time, only drink the liquids on the list below. Do not eat or drink anything else. Stop drinking 2 hours before your arrival time.
- Water.
- Clear apple juice, clear grape juice, or clear cranberry juice.
- Gatorade or Powerade.
-
Black coffee or plain tea. It’s OK to add sugar. Do not add anything else.
- Do not add any amount of any type of milk or creamer. This includes plant-based milks and creamers.
- Do not add flavored syrup.
If you have diabetes, pay attention to the amount of sugar in your drinks. It’s easier to control your blood sugar levels if you include sugar-free, low-sugar, or no added sugar versions of these drinks.
It’s helpful to stay hydrated before surgeries and procedures, so drink if you’re thirsty. Do not drink more than you need. You’ll get intravenous (IV) fluids during your surgery or procedure.
Stop drinking 2 hours before your arrival time. This includes water.
Your healthcare provider may have given you different instructions for when to stop drinking. If so, follow their instructions.
What to bring
- A list of all the medicines you take at home, including prescription and over-the-counter medicines, patches, and creams.
- Medicines for breathing problems (such as your inhaler), medicines for chest pain, or both.
- Your cell phone and charger.
- A case for your personal items, if you have any. Eyeglasses or contacts, hearing aids, dentures, prosthetic devices, wigs, and religious articles are examples of personal items.
- Your Health Care Proxy form and other advance directives, if you filled them out.
- Your breathing device for sleep apnea (such as your CPAP machine), if you use one. If you cannot bring it, we will give you one to use while you’re at the hospital.
What to expect when you arrive
Many doctors, nurses, and other staff members will ask you to say and spell your name and date of birth. This is for your safety. People with the same or similar names may be having procedures on the same day.
Once you’re brought to the presurgical area, you’ll get a hospital gown and nonskid socks to wear. You’ll take off your eyeglasses, hearing aids, dentures, prosthetic devices, wig, and religious articles.
Meet with a nurse
You’ll meet with a nurse before your procedure. Tell them the dose of any medicines you took after midnight (12 a.m.) and the time you took them. Make sure to include prescription and over-the-counter medicines, patches, and creams.
Your nurse will place an intravenous (IV) line into a vein in your arm or hand, unless you already have:
- A central venous catheter (CVC) or any other type of central line.
- A peripherally inserted central catheter (PICC).
- An implanted port (also called a mediport or Port-A-Cath).
You’ll be under sedation for your procedure. When you’re under sedation, you’ll get a sedative. This is medicine that makes you sleepy and relaxed during your procedure. A member of your care team will review your medical history with you to get you ready for sedation.
They will:
- Ask you if you’ve had any problems with sedation in the past. This includes nausea (feeling like you’re going to throw up) or pain.
- Talk with you about your comfort and safety during your procedure.
- Talk with you about the kind of sedation you’ll get.
- Answer any questions you may have about sedation.
What to expect during your procedure
When it’s time for your procedure, you’ll be brought into the procedure room and helped onto the table. You’ll lie flat on your back.
A member of your care team may put compression boots on your lower legs. These gently inflate and deflate to help blood flow in your legs. You’ll be attached to equipment to monitor (keep track of) your heart rate, breathing, and blood pressure. You’ll also get oxygen through a thin tube that rests below your nose.
You will be given sedation and you’ll feel relaxed or even sleepy.
During your procedure
A member of your care team will clean the skin in the area where your IR doctor will be working. This area is called the insertion site. The insertion site will be in your groin (the area between your belly and thigh). In some cases, the insertion site may be in your wrist. A member of your care team will also shave the insertion site, if needed.
You’ll get an injection (shot) of a local anesthetic to numb the insertion site. Then, your IR doctor will put a needle into an artery in the numbed area. They’ll thread a catheter through the needle into the artery.
Your IR doctor will guide the catheter until it reaches the smaller arteries that supply blood to your prostate. They’ll use live X-ray pictures and contrast injections to guide the catheter to the right place.
The contrast dye will help them see the blood vessels that go to your prostate in the pictures. This is called an arteriogram (ar-TEER-ee-oh-gram).
Once the catheter is in the main blood vessel that goes to your prostate, your IR doctor will start the embolization. They’ll inject an embolic (blocking) agent into the catheter. These are tiny particles, each the size of a grain of sand.
The particles will move through the catheter into the smaller arteries that supply blood to your prostate. The particles will plug up these arteries, blocking blood flow to your prostate. This will make your prostate shrink.
When the procedure is done, your IR doctor will take out the catheter. They’ll use a small closure device to stop any bleeding from the insertion site. It is the size of a hole at the end of a pen. Then, a member of your care team will clean the insertion site. They’ll cover it with a small dressing (bandage), such as a Band-Aid®.
This procedure takes about 2 to 3 hours.
What to expect after your procedure
After your procedure, you’ll be brought to the Post-Anesthesia Care Unit (PACU). While you’re in the PACU, tell your nurse if your dressing feels wet or warm.
Your nurse will monitor how you are feeling after your procedure. They’ll also monitor the insertion site for any bleeding.
You’ll be in the PACU for 1 to 4 hours before you’re discharged home with your responsible care partner. You must urinate before you leave.
Most people feel only mild discomfort in the groin area, around the insertion site. Your IR doctor will send prescriptions to your pharmacy in case you need them. The prescriptions will be for:
- Pain medicine
- Antinausea medicine (medicine to keep you from feeling like you’re going to throw up).
- Anti-inflammatory medicine (medicine that reduces pain, fever, and swelling)
- Medicine to reduce bladder irritation or bladder spasms.
You will have 2 follow-up appointments with your IR doctor. The first appointment will be about 2 to 4 weeks after your procedure. The second appointment will be about 3 months after your procedure.
What to do at home after your prostate artery embolization
- You can take off your dressing the day after your procedure.
- Do not shower or bathe for the first 24 hours (1 day) after your procedure. You can shower or bathe like you normally do after that.
- Do not lift anything heavier than 10 pounds (4.5 kilograms) 3 days after your procedure.
- Do not exercise for 1 week after your procedure.
-
Do not ejaculate for 1 week after your procedure.
- Your first ejaculation may have some blood. This is normal and will go away with time.
-
Do not work for 1 week after your procedure if you lift heavy objects or do heavy physical activity at your job.
- For some jobs, you can go back to work the day after your procedure. This is OK if you sit at a desk or don’t do a lot of physical activity at work.
- Follow your IR doctor’s instructions when taking your medicines. Some of the medicines may make your urine an orange color. This is normal.
- You may notice some blood in your urine for a few days after your procedure. This is normal and will go away with time.
- You may need to urinate more often for 7 to 10 days after your procedure. This is normal.
- You may have pain and burning when urinating for up to 7 days after your procedure. If you do, take the medicines your IR doctor prescribed to treat this. This is normal and will get better on its own with time.
- Keep taking all of the prostate medicines you were taking before your procedure. Once you recover, talk with your IR doctor at your follow-up appointment. Ask them if you can change the dose (amount) or stop taking your prostate medicines.
When to call your healthcare provider
Call your IR doctor if you:
- Have a fever of 100.4° F (38° C) or higher.
- Have pain, nausea (feeling like you’re going to throw up), or vomiting (throwing up) that will not stop.
- Have pain, nausea, or vomiting that’s worse than it was before your procedure.
- Have redness, swelling, or bleeding around the insertion site.
- Cannot urinate.
- Have any symptoms that are worrying you.
Learn about our Health Information Policy.