This information describes fertility preservation options for people born with ovaries and a uterus. It’s meant for people who have not yet started cancer treatment. It explains:
- How cancer treatment may affect your fertility (ability to get pregnant).
- How you may be able to preserve your fertility before beginning treatment.
In this resource, we use the word “female” to refer to people born with ovaries and a uterus.
Basic reproductive biology
Understanding basic reproductive biology can be helpful as you make decisions about your fertility.
Ovulation
The female reproductive system has several parts (see Figure 1).
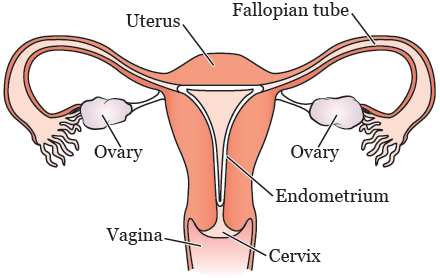
Your ovaries have 2 functions:
- They produce hormones (estrogen and progestin).
- They hold your eggs (oocytes). Each egg is contained in a sac called a follicle.
When you start puberty, your pituitary gland (located in your brain) releases hormones that cause a group of follicles to grow each month. The egg inside each growing follicle starts to mature. As the follicles grow, the ovary releases hormones that cause the lining of your uterus (endometrium) to thicken and prepare for a pregnancy.
One egg from the group of growing follicles fully matures each month. It’s released from one of your ovaries into the fallopian tube. This process is called ovulation. The other follicles growing that month break down and the eggs are cleared from the body. Through this monthly process, females lose many eggs over time.
Pregnancy
If you’re not using birth control and you have vaginal sex with a male partner around the time you’re ovulating, a single sperm may fertilize the egg. The fertilized egg begins to divide, forming an embryo. If the embryo implants in your endometrium, you become pregnant. The cells of the embryo continue to divide, becoming a fetus. During pregnancy, your uterus expands to hold the fetus as it grows.
Menstruation
If the egg released during ovulation doesn’t become fertilized, or if the embryo doesn’t implant in the endometrium, hormone levels drop and cause the lining of the uterus to shed. This bloody discharge forms your monthly menstrual period. The cycle then begins again, with new eggs maturing each month.
Ovarian reserve
Females are born with about 1 million eggs. During a female’s lifetime, only 400 to 500 eggs are released during ovulation. The other eggs die naturally over time, so the number of eggs in the ovaries (called the ovarian reserve) gradually gets lower (see Figure 2). With fewer eggs, it’s harder to become pregnant. Eventually, there are so few eggs that a female becomes infertile (unable to get pregnant).
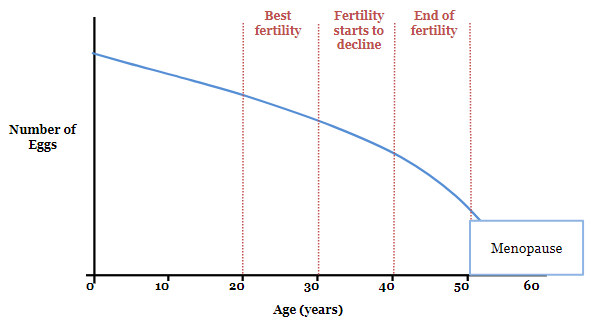
Menopause
With the loss of eggs, the ovaries stop producing hormones. This causes monthly menstrual periods to stop. When a female’s menstrual periods stop, this is called menopause. Most females lose their fertility 5 to 10 years before menopause. This is because of the loss of eggs and because the quality of their eggs declines over time.
Effects of cancer treatment on fertility
Cancer treatments can affect fertility in a number of ways.
-
Some chemotherapy medications destroy eggs. This decrease in the number of eggs may lead to infertility after treatment.
- The risk of infertility depends on the medications used, the doses given, and the age of the female at the time of treatment. Older females have fewer eggs when they start treatment. This means they are more likely to become infertile after treatment.
- This loss of eggs in the ovaries from chemotherapy can reduce the chance of pregnancy in the same way that natural aging does. Some females lose so many eggs that they become infertile and begin menopause right after treatment. Some females still have eggs remaining after treatment but may develop infertility and menopause at a young age. This narrows the window of time that a female can become pregnant.
-
Radiation therapy to the pelvis or whole abdomen (belly) destroys eggs in a similar way to chemotherapy. Radiation may also damage the uterus, causing fibrosis (scarring).
- Depending on the dose of radiation to the uterus, females may not be able to become pregnant after radiation. Females who do become pregnant may not be able to safely carry a pregnancy because their uterus may not be able to expand with a growing fetus. This can make you more likely to have a miscarriage or premature labor.
- Surgery or radiation therapy to the brain may affect the pituitary gland, which releases hormones that stimulate egg maturation and ovulation. However, this doesn’t damage the eggs in the ovaries. There are medications that replace these hormones that may help you become pregnant.
- Surgery involving a single ovary, both ovaries, or the uterus can affect fertility.
Because of the many factors that can affect fertility, it’s hard to know how you may be affected by your treatment. We can’t know for sure who will still be able to get pregnant after treatment is finished and who will not. We also can’t know for sure how long a female will be fertile after treatment. If you have questions about your risk of infertility based on the treatment you will receive, speak with your oncologist (cancer doctor).
Fertility preservation options
A number of options are available that may preserve your fertility and increase the chance you will be able to have a biologic child in the future. Not all females starting cancer treatment will need or want to consider these options.
The decision whether to pursue fertility preservation is a personal one. We want you to know what options are available. This will allow you to have all the information that you need to make the best decision for yourself so that you can avoid regret in the future.
Fertility preservation options for females include:
- Egg or embryo freezing
- Ovarian tissue freezing
- Ovarian suppression
- Ovarian transposition
- Alternative treatment for certain early stage gynecologic cancers
Egg or embryo freezing
Egg and embryo freezing are procedures in which mature eggs are removed from your ovary to be frozen and stored for possible use in the future. They can be frozen as unfertilized eggs or fertilized with sperm and frozen as embryos. These procedures are performed by specially trained gynecologists, called reproductive endocrinologists (RE). We don’t have REs at MSK, but we can make a referral for you.
The process of egg or embryo freezing takes about 2 weeks. There are several steps involved, including:
-
Evaluation: Your RE will do a number of tests to help determine how successful egg or embryo freezing may be for you. They will also want to speak with your oncologist to make sure it’s safe for you to undergo egg or embryo freezing. The tests you have may include:
- A transvaginal ultrasound, in which a thin wand is placed in your vagina. Sound waves from the wand create pictures of your ovaries and uterus. With this test, your doctor can examine your ovaries and count the number of large growing follicles in your ovaries. This is called the antral follicle count. If you’ve never had a gynecologic exam or vaginal sex, your RE may be able to perform the ultrasound using a wand placed on your abdomen rather than in your vagina.
- Blood tests to measure the levels of hormones related to fertility, including follicle stimulating hormone (FSH) and anti-mullerian hormone (AMH).
-
Ovarian stimulation: If you decide to proceed, you will need to give yourself hormone injections (shots) each day for about 10 days. A nurse at the fertility center will teach you how to do this. These hormones will stimulate multiple eggs in your ovaries to mature. You don’t need to be at any particular phase in your menstrual cycle to begin.
- During this period of stimulation, you will see the RE almost every other day for blood tests and ultrasounds. These tests show how your ovaries are responding to the hormones. If needed, your RE may change the doses of the hormones. Once your eggs are fully mature, the egg retrieval will be scheduled.
-
Egg retrieval: This is an outpatient procedure, done with anesthesia (medication to make you sleep), so you won’t feel pain. You don’t need an incision (surgical cut).
- Once you’re asleep, an ultrasound wand is be placed in your vagina so your RE can see your ovaries. A very thin needle is passed through the wall of your vagina up to your ovary to collect the mature eggs (see Figure 3).
- The entire procedure takes about 20 minutes and most females are discharged within 1 hour.
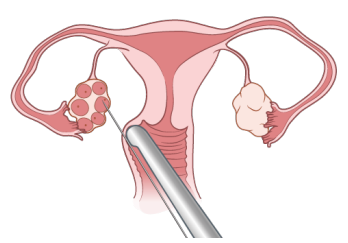
Figure 3. Egg retrieval
Once the eggs are retrieved, they will be frozen for your future use. The eggs can be frozen unfertilized or after they are fertilized with sperm to create embryos (in- vitro fertilization). Eggs and embryos can be stored for as long as you want.
Before beginning egg or embryo freezing, talk with your oncologist to be sure you can take the time to do this and that the procedure is safe for you. Most patients only do 1 cycle of stimulation before their cancer treatment. However, the more eggs you’re able to freeze, the greater the chance that you will be successful in having a baby using these eggs in the future.
Depending on how many mature eggs or embryos you’re able to freeze, your RE may suggest you undergo a second cycle. If you’re considering a second cycle, speak with your oncologist first to be sure this will not delay your cancer treatment longer than is safe for you.
Considerations for females with breast cancer
The hormone medication needed to stimulate your eggs to mature will cause your estrogen levels to rise for 2 to 3 weeks. To lower estrogen levels, we generally recommend that females with breast cancer take a medication called letrozole during stimulation, and for 1 to 2 weeks after the eggs are collected. Your RE will discuss this with you and prescribe the medication.
We can’t say for certain if this short period of estrogen exposure is safe, but there have been no reports that females with breast cancer who undergo egg or embryo freezing are more likely to have the cancer return. Everyone’s situation is different and we encourage you to speak with your oncologist if you’re considering this.
Also, females with estrogen receptor positive breast cancer often need to take endocrine therapy for up to 10 years after finishing chemotherapy or radiation therapy. It isn’t safe to become pregnant while on this treatment because there is a risk of birth defects. Most females with estrogen receptor positive breast cancer are advised to wait 10 years before attempting pregnancy. If you’re considering interrupting endocrine therapy to try to get pregnant before 10 years are up, discuss this with your oncologist. To learn more, read Pregnancy After Treatment for Early Stage Breast Cancer.
Cost of egg and embryo freezing
Freezing eggs and embryos is costly, and unfortunately, many health insurance plans don’t cover the cost. This may change in the future. Every fertility center charges a different amount, but most centers offer discounted rates to patients starting cancer treatment.
There are additional costs for the hormone medication needed for ovarian stimulation. If your prescription plan doesn’t cover the medications, there are programs that may help:
-
LIVESTRONG Fertility works with a pharmaceutical company to provide free medication to patients being treated at participating fertility centers. Eligibility is based on your income.
- To learn more go to www.livestrong.org/we-can-help/livestrong-fertility
- To get an application, go to https://livestrongfertilityportal.unicentric.com/Login/Index#. You must submit the application and obtain approval before you start ovarian stimulation. To speak directly with one of their navigators, call 855-844-7777.
- Heartbeat is a program that offers free medication through a pharmaceutical company and Walgreens. To learn more, go to: www.walgreens.com/images/adaptive/pharmacy/specialty-pharmacy/Preserving+the+Future-Patient_WEB+09-05-12.pdf. Ask your RE if you’re eligible and if they can apply for you.
There will be an annual storage fee to keep your eggs or embryos frozen. There are also additional costs when you’re ready to thaw and use the eggs or embryos to attempt pregnancy. A financial specialist at the fertility center can determine what if anything will be covered by your health insurance and what you will have to pay yourself.
How frozen eggs and embryos are used to attempt pregnancy
If you use your frozen eggs or embryos in the future, they will be thawed when you’re ready to attempt pregnancy. If you froze eggs, they will be fertilized with sperm to create embryos.
If you no longer have regular periods, or are in menopause from your treatment, you will need to take hormones for several weeks to prepare the lining of your uterus for pregnancy. The embryos will be transferred into your uterus. The embryos are drawn up into a very thin, soft catheter that is passed through your vagina and cervix into your uterus. The embryos are released and the catheter is taken out. The procedure is done in an exam room. It does not hurt, so you will not need anesthesia.
If you’re not able to carry a pregnancy yourself, the embryos can be transferred to the uterus of another female to carry the pregnancy for you. This is called surrogacy with a gestational carrier.
About 2 weeks after the embryo transfer, a blood test is done to see if you, or your gestational carrier, have become pregnant. If the pregnancy test is positive, an ultrasound will be done several weeks later to see if the embryo has implanted to confirm the pregnancy. You will then schedule an appointment with an obstetrician (a doctor who specializes in pregnancy and childbirth) who will care for you during the pregnancy. You may need to continue taking hormones for several months to support the pregnancy.
If the embryo did not implant, and you have other embryos being stored, your RE can perform another embryo transfer when you’re ready.
Success rates with frozen eggs and embryos
The chance that you will be successful in having a baby using frozen eggs or embryos depends on your age at the time of egg retrieval and the number of mature eggs obtained from the procedure. Not every egg collected can become a baby. Some eggs will not survive the freeze-thaw cycle, some will not fertilize and develop into embryos, and some may not implant after the transfer. Females under 35 years of age generally have a higher chance of success. Discuss your personal chance of success with your RE after your initial evaluation.
Ovarian tissue freezing
Some females will not be able to undergo egg or embryo freezing due the urgent need to begin treatment. They may have the option to preserve fertility with ovarian tissue freezing. This is an experimental procedure in which an entire ovary, or pieces of an ovary, are removed during a surgery. The ovarian tissue is brought to a special laboratory to be processed. The outer layer of the ovary, which holds the eggs, will be removed, cut into small pieces, and frozen. A small amount of the tissue will be used for research to find the best way to help females have children using ovarian tissue. The rest of the tissue will be stored for your personal use.
Currently, the option for using this tissue in the future is to re-implant it into your body, with the hope that eggs in the tissue will mature and be released with ovulation. As of 2019, about 130 babies have been born worldwide after re-implantation of ovarian tissue. Another option for using this tissue is to stimulate the eggs to mature in the laboratory (in vitro maturation), The mature eggs could then be fertilized to create embryos for transfer to your uterus. No babies have yet been born using this technique. To learn more about ovarian tissue, read About Ovarian Tissue Freezing. Ovarian tissue freezing may not be an option for all females. If you would like to learn more, ask your oncologist to refer you to a RE who performs ovarian tissue freezing.
Ovarian suppression
Ovarian suppression involves taking monthly injections of a medication called leuprolide to block hormones that stimulate your ovaries. This prevents eggs from maturing, with the hope that this will protect them from the effects of chemotherapy.
The injections usually start 1 to 2 weeks before the first chemotherapy treatment and continue until your treatment is completed. Side effects of the medication may include symptoms similar to those of menopause, such as hot flashes, mood changes, difficulty sleeping, and vaginal dryness. These side effects will stop after you stop taking the medication. If it’s safe for you to take hormones, low-dose birth control pills can be prescribed to prevent these symptoms.
Ovarian suppression has been studied mostly in females with breast cancer and lymphoma. Based on the results of these studies it can be considered reasonable for all premenopausal females who will receive chemotherapy to consider it as an option to reduce the chances of premature menopause. Females who are interested in fertility preservation to have a child in the future, however, could consider ovarian suppression after freezing their eggs. If you want to consider this option, speak with your oncologist.
Ovarian transposition
Ovarian transposition may be an option if you’re receiving radiation therapy to the pelvis. This is a surgical procedure that moves your ovaries out of the field of treatment. This will lower the amount of radiation your ovaries are exposed to during your treatment and may help your ovaries keep working properly after treatment. The surgery is done through several small incisions in your abdominal wall. For more information ask your nurse for the resource About Your Ovarian Transposition Surgery or search for it on www.mskcc.org/pe. If you’re interested in ovarian transposition, ask your radiation oncologist to refer you to a gynecologic surgeon here at MSK.
Alternative treatment for certain early-stage gynecologic cancers
For females with certain early-stage gynecologic cancers, it may be possible to do limited surgery, or in some cases take medication to preserve fertility. For example, some females who have early-stage cervical cancer can have their cervix removed but have their uterus left in place. This procedure is called radical trachelectomy and may help you carry a pregnancy. To learn more about radical trachelectomy, read About Your Radical Trachelectomy.
Not all females are eligible for these limited surgeries. It depends on the location and size of your tumor. If you’re interested, ask your gynecologic surgeon if you’re a candidate.
Other options for building a family
Some females will not be able to preserve their fertility before treatment and some may choose not to for personal reasons. This doesn’t necessarily mean that you won’t be able to build a family. Some females will be able to get pregnant naturally without medical help. Some may have a low ovarian reserve but will be able to get pregnant with fertility treatment provided by a RE. If you’re unable to have a biological child in the future, there are other ways of building a family after cancer treatment.
- You can use donor eggs or embryos. Donor eggs are given by young females who undergo a cycle of ovarian stimulation and egg retrieval. These are fertilized with sperm from your partner or a donor to create embryos for transfer into your uterus. Donor embryos are usually given by couples who had infertility treatment, have completed building their families, and do not want to discard their remaining embryos. The cost of using donor embryos is much lower than that of donor eggs.
- You can adopt. Having a history of cancer doesn’t prevent you from being able to adopt as long as you’re healthy and have been cancer-free for several years.
To learn more about these options, read Building Your Family After Cancer Treatment: For People Born With Ovaries and a Uterus.
Additional resources
A number of resources are available to help you learn more and make a decision about fertility preservation. First, speak with your oncologist to make sure that it’s safe for you to pursue fertility preservation. If you would like more information about the options available, or support as you consider these issues, ask your oncologist to refer you to one of our Fertility Nurse Specialists.
In addition, the organizations listed below have information about fertility preservation that may be helpful to you.
American Cancer Society
Fertility and Women with Cancer
www.cancer.org/treatment/treatments-and-side-effects/physical-side-effects/fertility-and-sexual-side-effects/fertility-and-females-with-cancer.html
CancerNet
Fertility Concerns and Preservation for Women
www.cancer.net/coping-and-emotions/sexual-and-reproductive-health/fertility-concerns-and-preservation-females
LIVESTRONG/Fertility
www.livestrong.org/we-can-help/livestrong-fertility
Oncofertility Consortium of Northwestern University: Save My Fertility
www.savemyfertility.org

