This guide will help you get ready for your total laryngectomy at MSK. It will also help you understand what to expect during your recovery.
Use this guide as a source of information in the days leading up to your surgery. Bring it with you on the day of your surgery. You and your care team will refer to it as you learn more about your recovery.
About your total laryngectomy
About your larynx (voice box)
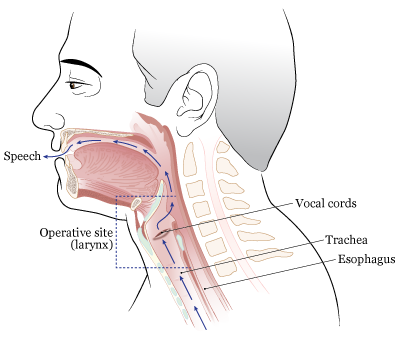
Your larynx is in your neck above your trachea (windpipe). It’s the entrance to your airway and is important in breathing, swallowing, and speaking.
When you breathe, your larynx opens to let air reach your lungs.
When you swallow, your larynx rises and closes your airway to keep food and liquid from getting in your lungs.
Two muscular folds in your larynx, called your vocal folds or vocal cords, vibrate to make your speaking voice.
About your total laryngectomy
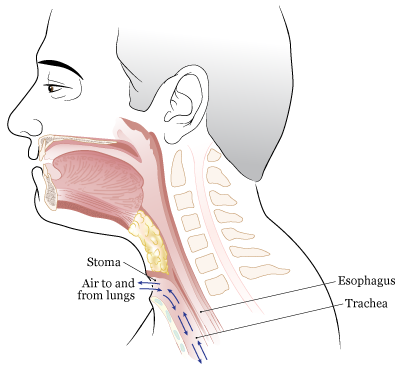
A total laryngectomy is a surgery to remove your whole larynx (see Figures 1 and 2).
After your surgery, you’ll need to adjust how you speak and breathe.
- You’ll need to learn a new way to speak. You’ll meet with a speech pathologist before your surgery. They’ll review how your airway will be different after your surgery. They’ll also talk with you about ways to speak after your laryngectomy and show you a video demonstrating these ways.
- Your nose and mouth will no longer be connected to your trachea. You’ll breathe through a new opening in your neck called a stoma. Air will pass through the stoma into and out of your lungs. This will be your only way to breathe. You’ll be a “neck breather” and, if you need CPR, it’ll need to be given mouth-to-neck.
Your incisions (surgical cuts) will be closed with plastic or nylon sutures (stitches). The sutures will stay in place for about 2 weeks. They may be removed at your post-operative visit with your surgeon. If you’ve had radiation therapy to the area, they may need to stay in place for longer.
The length of your surgery depends on which type of surgery and incisions you have. Your surgeon will talk with you about this before your surgery.
We recognize that your upcoming surgery is life changing. Your care team at MSK will help you through the process.
Before your total laryngectomy
This section will help you get ready for your surgery. Read it when your surgery is scheduled. Refer to it as your surgery gets closer. It has important information about what to do to get ready.
As you read this section, write down questions to ask your healthcare provider.
Getting ready for surgery
You and your care team will work together to get ready for your surgery. Help us keep you safe by telling us if any of these things apply to you, even if you’re not sure.
You may need to follow special instructions before surgery based on the medicines and supplements you take. If you do not follow those instructions, your surgery may be delayed or canceled.
-
I take any prescription medicines. A prescription medicine is one you can only get with a prescription from a healthcare provider. Examples include:
- Medicines you swallow.
- Medicines you take as an injection (shot).
- Medicines you inhale (breathe in).
- Medicines you put on your skin as a patch or cream.
- I take any over-the-counter medicines, including patches and creams. An over-the-counter medicine is one you can buy without a prescription.
- I take any dietary supplements, such as herbs, vitamins, minerals, or natural or home remedies.
- I have a pacemaker, automatic implantable cardioverter-defibrillator (AICD), or other heart device.
- I have had a problem with anesthesia (A-nes-THEE-zhuh) in the past. Anesthesia is medicine to make you sleep during a surgery or procedure.
- I’m allergic to certain medicines or materials, including latex.
- I’m not willing to receive a blood transfusion.
- I use recreational drugs, such as marijuana.
GLP-1 medicines for weight loss
You may be taking a GLP-1 medicine. If so, it’s important to tell your healthcare provider. You will need to follow special eating and drinking instructions before your surgery or procedure. It is very important to follow these instructions. If you do not follow them, your surgery or procedure may be delayed or canceled.
- Follow a clear liquid diet the day before your surgery or procedure. Do not eat any solid food. Read Clear Liquid Diet to learn more.
- Stop drinking 8 hours before your arrival time. Do not eat or drink anything after this time, including clear liquids. You can have small sips of water with your medicines.
To learn more, read Eating and Drinking Before Your Surgery or Procedure When Taking GLP-1 Medicines.
Here are some examples of GLP-1 medicines. There are others, so be sure your care team knows all the medicines you take. Sometimes, these are prescribed to help manage diabetes or other conditions. Other times, they’re prescribed for weight loss.
|
|
About drinking alcohol
It’s important to talk with your healthcare providers about how much alcohol you drink. This will help us plan your care.
If you drink alcohol regularly, you may be at risk for problems during and after your surgery. These include bleeding, infections, heart problems, and a longer hospital stay.
If you drink alcohol regularly and stop suddenly, it can cause seizures, delirium, and death. If we know you’re at risk for these problems, we can prescribe medicine to help prevent them.
Here are things you can do before your surgery to keep from having problems.
- Be honest with your healthcare providers about how much alcohol you drink.
-
Try to stop drinking alcohol once your surgery is planned. Tell your healthcare provider right away if you:
- Get a headache.
- Feel nauseous (like you’re going to throw up).
- Feel more anxious (nervous or worried) than usual.
- Cannot sleep.
These are early signs of alcohol withdrawal and can be treated.
- Tell your healthcare provider if you cannot stop drinking.
- Ask your healthcare provider questions about drinking and surgery. All your medical information will be kept private, as always.
About smoking
If you smoke or use an electronic smoking device, you can have breathing problems when you have surgery. Vapes and e-cigarettes are examples of electronic smoking devices. Stopping for even a few days before surgery can help prevent breathing problems during and after surgery.
Your healthcare provider will refer you to our Tobacco Treatment Program if you smoke. You can also reach the program by calling 212-610-0507.
About sleep apnea
Sleep apnea is a common breathing problem. If you have sleep apnea, you stop breathing for short lengths of time while you’re asleep. The most common type is obstructive sleep apnea (OSA). With OSA, your airway becomes fully blocked during sleep.
OSA can cause serious problems during and after surgery. Tell us if you have or think you might have sleep apnea. If you use a breathing device, such as a CPAP machine, bring it on the day of your surgery.
Using MSK MyChart
MSK MyChart (mskmychart.mskcc.org) is MSK’s patient portal. You can use it to send and read messages from your care team, view your test results, see your appointment dates and times, and more. You can also invite your caregiver to make their own account so they can see information about your care.
If you do not have an MSK MyChart account, you can sign up at mskmychart.mskcc.org. You can also ask a member of your care team to send you an invitation.
If you need help with your account, call the MSK MyChart Help Desk at 646-227-2593. They are available Monday through Friday between and (Eastern time).
Within 30 days of your surgery
Presurgical Testing (PST)
You’ll have a PST appointment before your surgery. You’ll get a reminder from your surgeon’s office with the appointment date, time, and location. Visit www.msk.org/parking for parking information and directions to all MSK locations.
You can eat and take your usual medicines the day of your appointment.
It’s helpful to bring these things to your appointment:
- A list of all the medicines you’re taking, including prescription and over-the-counter medicines, patches, and creams.
- Results of any medical tests done outside of MSK in the past year, if you have them. Examples include results from a cardiac stress test, echocardiogram, or carotid doppler study.
- The names and telephone numbers of your healthcare providers.
You’ll meet with an advance practice provider (APP) during your PST appointment. They work closely with MSK’s anesthesiology (A-nes-THEE-zee-AH-loh-jee) staff. These are doctors with special training in using anesthesia during a surgery or procedure.
Your APP will review your medical and surgical history with you. You may have tests to plan your care, such as:
- An electrocardiogram (EKG) to check your heart rhythm.
- A chest X-ray.
- Blood tests.
Your APP may recommend you see other healthcare providers. They’ll also talk with you about which medicines to take the morning of your surgery.
Identify your caregiver
Your caregiver has an important role in your care. Before your surgery, you and your caregiver will learn about your surgery from your healthcare providers. After your surgery, your caregiver will take you home when you’re discharged. They’ll also help you care for yourself at home.
For caregivers
Caring for a person going through cancer treatment comes with many responsibilities. We offer resources and support to help you manage them. Visit www.msk.org/caregivers or read A Guide for Caregivers to learn more.
Fill out a Health Care Proxy form
If you have not already filled out a Health Care Proxy form, we recommend you do now. If you already filled one out or have any other advance directives, bring them to your next appointment.
A health care proxy is a legal document. It says who will speak for you if you cannot communicate for yourself. This person is called your health care agent.
- To learn about health care proxies and other advance directives, read Advance Care Planning for People With Cancer and Their Loved Ones.
- To learn about being a health care agent, read How to Be a Health Care Agent.
Talk with a member of your care team if you have questions about filling out a Health Care Proxy form.
7 days before your surgery
Follow your healthcare provider’s instructions for taking aspirin
Aspirin can cause bleeding. If you take aspirin or a medicine that has aspirin, you may need to change your dose or stop taking it 7 days before your surgery. Follow your healthcare provider’s instructions. Do not stop taking aspirin unless they tell you to.
To learn more, read How To Check if a Medicine or Supplement Has Aspirin, Other NSAIDs, Vitamin E, or Fish Oil.
Stop taking vitamin E, multivitamins, herbal remedies, and other dietary supplements
Vitamin E, multivitamins, herbal remedies, and other dietary supplements can cause bleeding. Stop taking them 7 days before your surgery. If your healthcare provider gives you other instructions, follow those instead.
To learn more, read Herbal Remedies and Cancer Treatment.
2 days before your surgery
Stop taking nonsteroidal anti-inflammatory drugs (NSAIDs)
NSAIDs, such as ibuprofen (Advil® and Motrin®) and naproxen (Aleve®), can cause bleeding. Stop taking them 2 days before your surgery. If your healthcare provider gives you other instructions, follow those instead.
To learn more, read How To Check if a Medicine or Supplement Has Aspirin, Other NSAIDs, Vitamin E, or Fish Oil.
1 day before your surgery
Note the time of your surgery
A staff member will call you after the day before your surgery. If your surgery is scheduled for a Monday, they’ll call you the Friday before. If you do not get a call by , call 212-639-5014.
The staff member will tell you what time to get to the hospital for your surgery. They’ll also remind you where to go.
This will be one of the following locations:
-
Presurgical Center (PSC) on the 2nd floor
1275 York Avenue (between East 67th and East 68th Streets)
New York, NY 10065
Take the M Elevator to the 2nd floor. -
Presurgical Center (PSC) on the 6th floor
1275 York Avenue (between East 67th and East 68th Streets)
New York, NY 10065
Take the B elevator to the 6th floor.
Visit www.msk.org/parking for parking information and directions to all MSK locations.
Instructions for eating
Stop eating at midnight (12 a.m.) the night before your surgery or procedure. This includes hard candy and gum.
Your healthcare provider may have given you different instructions for when to stop eating. If so, follow their instructions. Some people need to fast (not eat) for longer before their surgery or procedure.
The morning of your surgery
Instructions for drinking
Between midnight (12 a.m.) and 2 hours before your arrival time, only drink the liquids on the list below. Do not eat or drink anything else. Stop drinking 2 hours before your arrival time.
- Water.
- Clear apple juice, clear grape juice, or clear cranberry juice.
- Gatorade or Powerade.
-
Black coffee or plain tea. It’s OK to add sugar. Do not add anything else.
- Do not add any amount of any type of milk or creamer. This includes plant-based milks and creamers.
- Do not add flavored syrup.
If you have diabetes, pay attention to the amount of sugar in your drinks. It’s easier to control your blood sugar levels if you include sugar-free, low-sugar, or no added sugar versions of these drinks.
It’s helpful to stay hydrated before surgeries and procedures, so drink if you’re thirsty. Do not drink more than you need. You’ll get intravenous (IV) fluids during your surgery or procedure.
Stop drinking 2 hours before your arrival time. This includes water.
Your healthcare provider may have given you different instructions for when to stop drinking. If so, follow their instructions.
Take your medicines as instructed
A member of your care team will tell you which medicines to take the morning of your surgery. Take only those medicines with a sip of water. Depending on what you usually take, this may be all, some, or none of your usual morning medicines.
Things to remember
- Don’t wear any lotion, cream, deodorant, makeup, powder, perfume, or cologne.
- If you wear contact lenses, wear your glasses instead. Wearing contact lenses during surgery can damage your eyes.
- Don’t wear any metal objects. Remove all jewelry, including body piercings. The tools used during your surgery can cause burns if they touch metal.
- Leave valuable items at home.
- If you’re menstruating (have your monthly period), use a sanitary pad, not a tampon. You’ll get disposable underwear, as well as a pad if needed.
What to bring
- A button-down or loose-fitting top.
- Your Health Care Proxy form and other advance directives, if you completed them.
- Your cell phone and charger.
- Only the money you may want for small purchases (such as a newspaper).
- A case for your personal items (such as eyeglasses, hearing aids, dentures, prosthetic devices, wig, and religious articles), if you have any.
- This guide. Your care team will use it to teach you how to care for yourself after surgery.
Once you’re in the hospital
Many staff members will ask you to say and spell your name and birth date. This is for your safety. People with the same or a similar name may be having surgery on the same day.
When it’s time to change for surgery, you’ll get a hospital gown, robe, and nonskid socks to wear.
Meet with a nurse
You’ll meet with a nurse before surgery. Tell them the dose of any medicines you took after midnight (12 a.m.) and the time you took them. Make sure to include prescription and over-the-counter medicines, patches, and creams.
Your nurse may place an intravenous (IV) line in one of your veins, usually in your arm or hand. If your nurse does not place the IV, your anesthesiologist (A-nes-THEE-zee-AH-loh-jist) will do it in the operating room.
Meet with an anesthesiologist
You’ll also meet with an anesthesiologist before surgery. They will:
- Review your medical history with you.
- Ask if you’ve had any problems with anesthesia in the past. This includes nausea (feeling like you’re going to throw up) or pain.
- Talk with you about your comfort and safety during your surgery.
- Talk with you about the kind of anesthesia you’ll get.
- Answer questions you have about anesthesia.
Get ready for surgery
When it’s time for your surgery, you’ll take off your eyeglasses, hearing aids, dentures, prosthetic devices, wig, and religious articles.
You’ll either walk into the operating room or a staff member will bring you there on a stretcher. A member of the operating room team will help you onto the operating bed. They’ll put compression boots on your lower legs. These gently inflate and deflate to help blood flow in your legs.
Once you’re comfortable, your anesthesiologist will give you anesthesia through your IV line and you’ll fall asleep. You’ll also get fluids through your IV line during and after your surgery.
During your surgery
After you’re fully asleep, a breathing tube will be placed through your mouth and into your windpipe to help you breathe. You’ll also have a nasogastric (NG) tube placed through your nose into your stomach to deliver food and a urinary (Foley) catheter placed to drain urine (pee) from your bladder.
Once your surgery is finished, your incisions will be closed with sutures (stitches). Your incisions may be covered with a bandage. Your breathing tube is usually taken out while you’re still in the operating room.
After your total laryngectomy
This section will help you know what to expect after your surgery. You’ll learn how to safely recover from your surgery both in the hospital and at home.
As you read this section, write down questions to ask your healthcare provider.
In the Post-Anesthesia Care Unit (PACU)
When you wake up after your surgery, you’ll be in the PACU. A nurse will be keeping track of your body temperature, pulse, blood pressure, and oxygen levels.
You’ll have a loose collar on your neck over your new stoma. This will deliver humidity and a small amount of extra oxygen to your lungs to keep the lining of your trachea moist. You’ll also have compression boots on your lower legs.
Pain medication
You’ll get IV pain medication while you’re in the PACU. You’ll be able to control your pain medication using a button called a patient-controlled analgesia (PCA) device. For more information, read the resource Patient-Controlled Analgesia (PCA).
Tubes and drains
You’ll have the following tubes:
- A laryngectomy tube in your stoma. This will help keep your laryngectomy stoma from closing.
- An NG tube in your nose. This will carry food and medications to your stomach.
- A Foley catheter in your bladder. This will let your care team keep track of how much urine you’re making.
Moving to your hospital room
Most people stay in the PACU overnight. After your stay in the PACU, a staff member will take you to your hospital room.
In your hospital room
The length of time you’re in the hospital after your surgery depends on your recovery. Most people stay in the hospital for 10 to 14 days.
When you’re taken to your hospital room, you’ll meet one of the nurses who will care for you while you’re in the hospital. They’ll explain how to control the lights and TV in your room and introduce you to other staff members who will help care for you during your stay.
Your nurse will also explain how to use the call bell system. It has an alert indicating you can’t speak. When you use the call bell, the person who answers will ask what you need. If no one is in your room to speak for you, a staff member will come to your room to help you.
Communicating
You’ll get a dry erase board to write on and a point-to-talk communication board to help you communicate. iPads are also available for your use.
About 3 to 5 days after your surgery, you’ll start using an electrolarynx to speak. About 2 to 3 weeks after your surgery, you can start learning to use other ways to speak, such as esophageal speech or tracheoesophageal speech. For more information about these communication options, read the section “Ways to communicate.”
Managing your pain
You’ll have some pain after your surgery. At first, you’ll get your pain medication through your IV line. You’ll be able to control your pain medication using a PCA device. Once you can get food through your NG tube, you’ll get your pain medication through your NG tube as well.
Your healthcare providers will ask you about your pain often and give you medication as needed. If your pain isn’t relieved, tell one of your healthcare providers. It’s important to control your pain so you can move around. Controlling your pain will help you recover better.
You’ll get a prescription for pain medication before you leave the hospital. Talk with your healthcare provider about possible side effects and when to start switching to over-the-counter pain medications.
Moving around and walking
Moving around and walking will help lower your risk for blood clots and pneumonia (lung infection). It will also help you start passing gas and having bowel movements (pooping) again. Your nurse, physical therapist, or occupational therapist will help you move around, if needed.
Eating and drinking
While you have an NG tube
You’ll start getting water and nutrients through your NG tube the day after your surgery.
Your NG tube will be removed once you can swallow liquids. This usually happens 8 to 10 days after surgery. If you had chemotherapy, radiation therapy, or other treatments before your surgery, your NG tube may need to stay in place for longer. You may also have an x-ray to make sure you’ve healed enough and are ready to start swallowing safely.
After your NG tube is removed
Once your NG tube is removed, you’ll start by only drinking liquids. You’ll then slowly move on to puréed foods, then to soft solid foods, and eventually to solid foods. Your healthcare provider will tell you when and what types of liquids and food you can have based on how you’re healing.
About swallowing
Swallowing after a total laryngectomy is usually similar to the way you swallowed before your surgery. If you had trouble swallowing before your surgery, it may even be easier to swallow after surgery. At first, it might feel like food or liquid is sticking in your throat and not going down your esophagus. If this happens, you may need to use the back of your tongue to give the food a little extra push when you start to swallow.
Tell your healthcare provider if you’re having trouble swallowing. They’ll refer you to a specialist who can help you with your speech and swallowing.
Caring for your laryngectomy stoma
Right after your surgery, your nurse will care for your stoma. Over time, they’ll teach you how to suction and care for your stoma yourself.
Remember that you’ll be a neck breather, so you’ll need to keep your airway open to breathe. Suctioning your stoma will keep it free of secretions and mucus and allow air in and out of your lungs. Your nurse will teach you how to suction your stoma and how often to do this.
Using a heat and moisture exchanger (HME)
You’ll also need to keep your stoma and airway moist. The moisture will help you cough out secretions and mucus. It will also keep mucus from drying out and causing plugs that can block your breathing.
Before your surgery, your nose and upper airway warmed and moisturized the air you breathed. After your surgery, you’ll use a HME to moisturize the air you breathe through your stoma. A HME is a small round device that you put over your stoma. There are different types of HMEs. Your nurse will help you find the one that works best for you.
HMEs work best when you wear one all the time. While you’re in the hospital, use a HME or humidity collar as much as possible. We’ll also give you HMEs to use at home. Taking your HME out before you cough can help keep it clean.
Put a new HME on your laryngectomy tube every day. Inspect your HME often, at least 3 times per day, to make sure it’s clean. If your HME is dirty, wipe it clean or change it. Never rinse it under water.
It might seem like you have more mucus or are coughing more when you first start using an HME. This is normal. It might take a few days or weeks of using a HME before it seems to be helping. If you’ve been using a HME for 3 weeks and don’t feel like you’re making less mucus and coughing less, tell your healthcare provider.
Your laryngectomy tube
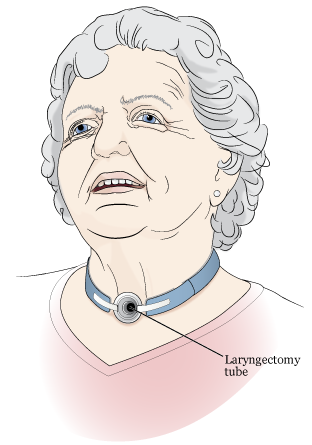
You’ll also get a soft plastic laryngectomy tube to keep the opening of your stoma from getting smaller (see Figure 3). Your healthcare provider will tell you how long you need to wear it.
Clean your laryngectomy tube regularly to help to keep it free of secretions. We recommend cleaning your tube at least twice a day or more as needed. Your nurse will show you how.
For instructions for caring for your stoma and cleaning your laryngectomy tube, read the section “Caring for and suctioning your laryngectomy stoma.”
Showering
Your healthcare provider will tell you when you can shower. For most people, this is at least 1 week after surgery.
Your nurse will give you a reusable shower shield to keep water from getting in your stoma when you shower. Bring it home when you’re discharged. Keep using it at home.
Don’t take baths or submerge yourself under water. If you do, too much water can enter your stoma. If this happens, you can drown.
Planning for your discharge
Before you leave the hospital, your case manager will meet with you to determine what kind of help you’ll need at home. This may include a visiting nurse to reinforce what you learned about caring for your stoma while you were in the hospital.
Your case manager will order a portable suction machine for you to use at home. The machine will be delivered to you while you’re still in the hospital. Your nurse will show you how to use it before you leave.
Your nurse will give you supplies so you can care for and suction your stoma for a couple of days after you’re discharged. We’ll also send you a kit that has the supplies you need for your laryngectomy. Depending on what you need, you may have more supplies delivered to your home. You should also find a medical supply store near your home.
Leaving the hospital
Before you leave, look at your incision with one of your healthcare providers. Knowing what it looks like will help you notice any changes later.
On the day of your discharge, plan to leave the hospital around Your healthcare provider will write your discharge order and prescriptions before you leave. You’ll also get written discharge instructions. One of your healthcare providers will review them with you before you leave.
If your ride isn’t at the hospital when you’re ready to leave, you may be able to wait in the Patient Transition Lounge. A member of your care team will give you more information.
At home
We strongly recommend registering with the MedicAlert® Foundation and wearing a MedicAlert ID with the words “Neck breather” on it. This way, if you stop breathing, medical personnel will know to give you oxygen through your neck instead of through your mouth. Visit www.medicalert.org to register.
Filling out your Recovery Tracker
We want to know how you’re feeling after you leave the hospital. To help us care for you, we’ll send questions to your MSK MyChart account. We’ll send them every day for 10 days after you’re discharged. These questions are known as your Recovery Tracker.
Fill out your Recovery Tracker every day before midnight (12 a.m.). It only takes 2 to 3 minutes to complete. Your answers to these questions will help us understand how you’re feeling and what you need.
Based on your answers, we may reach out to you for more information. Sometimes, we may ask you to call your surgeon’s office. You can always contact your surgeon’s office if you have any questions.
To learn more, read Common Questions About MSK's Recovery Tracker.
Managing your pain
People have pain or discomfort for different lengths of time. You may still have some pain when you go home and will probably be taking pain medication. Some people have soreness, tightness, or muscle aches around their incisions for 6 months or longer. This doesn’t mean something is wrong.
Follow these guidelines to help manage your pain at home.
- Take your medicines as directed and as needed.
- Call your healthcare provider if the medicine prescribed for you does not help your pain.
- Do not drive or drink alcohol while you’re taking prescription pain medicine. Some prescription pain medicines can make you drowsy (very sleepy). Alcohol can make the drowsiness worse.
-
You’ll have less pain and need less pain medicine as your incision heals. An over-the-counter pain reliever will help with aches and discomfort. Acetaminophen (Tylenol®) and ibuprofen (Advil or Motrin) are examples of over-the-counter pain relievers.
- Follow your healthcare provider’s instructions for stopping your prescription pain medicine.
- Do not take too much of any medicine. Follow the instructions on the label or from your healthcare provider.
- Read the labels on all the medicines you’re taking. This is very important if you’re taking acetaminophen. Acetaminophen is an ingredient in many over-the-counter and prescription medicines. Taking too much can harm your liver. Do not take more than one medicine that has acetaminophen without talking with a member of your care team.
- Pain medicine should help you get back to your usual activities. Take enough to do your activities and exercises comfortably. You may have a little more pain as you start to be more active.
- Keep track of when you take your pain medicine. It works best 30 to 45 minutes after you take it. Taking it when you first have pain is better than waiting for the pain to get worse.
Some prescription pain medications (such as opioids) may cause constipation (having fewer bowel movements than usual).
Preventing and managing constipation
Talk with your healthcare provider about how to prevent and manage constipation. You can also follow the guidelines below.
- Go to the bathroom at the same time every day. Your body will get used to going at that time. If you feel like you need to go, though, don’t put it off.
- Exercise, if you can. Walking is an excellent form of exercise.
- Drink 8 to 10 (8-ounce) glasses (2 liters) of liquids daily, if you can. Choose liquids such as water, juices (such as prune juice), soups, and ice cream shakes. Avoid liquids with caffeine (such as coffee and soda). Caffeine can pull fluid out of your body.
If you haven’t had a bowel movement in 2 days, call your healthcare provider.
Caring for and suctioning your laryngectomy stoma
You and your caregiver will need to learn how to suction and care for your new stoma. Remember that you’ll be a neck breather, so it’s important to keep your airway open so you can breathe. Suctioning your stoma will keep it free of secretions and allow air in and out of your lungs. Your nurse will teach you how to suction your stoma and how often to do this.
How to suction your laryngectomy stoma
-
Gather your supplies. You’ll need:
- A suction machine with plastic tubing
- A suction catheter
- A bowl or large cup filled with water
- A mirror
- A clean, dry cloth or paper towel (when you’re at home)
- Clean, dry gauze pads (when you’re in the hospital)
- Wash your hands well with soap and water.
- Connect the suction catheter to the suction machine’s plastic tubing.
- Place the mirror so you can see your laryngectomy stoma opening.
- Turn on the suction machine. (If you’re in the hospital, open the clamp on the suction tubing instead). Pinch the catheter between your thumb and pointer finger to block the suction.
- Cough deeply to bring up any secretions.
-
Keep the suction catheter pinched. Put it about 3 to 5 inches (8 to 13 centimeters) into your stoma (see Figure 4).
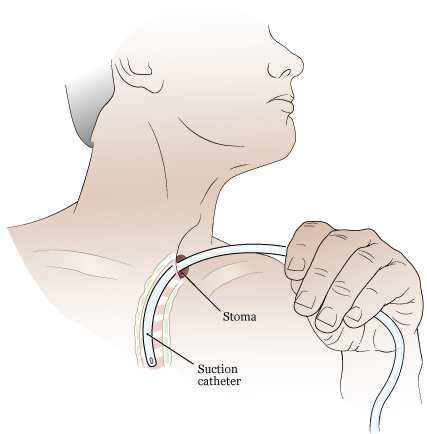
Figure 4. Suctioning your stoma - Un-pinch the catheter to start suctioning. Suction for 5 to 10 seconds or as long as directed by your healthcare provider. Don’t keep the catheter in your trachea for longer than 10 seconds. Keeping it in too long can cause shortness of breath.
- Using a rotating motion, slowly pull the suction catheter out of your stoma. Rotating the catheter helps it suck up secretions on all sides of your trachea and stoma.
- Wipe the secretions from the outside of the suction catheter with a clean, dry cloth or paper towel. (If you’re in the hospital, use dry gauze instead).
- Rinse the secretions from the inside of the suction catheter by suctioning water through it.
- Repeat these steps if you feel you have more secretions that need to be cleared out. If you need to repeat the suctioning more than 2 or 3 times, rest for a few minutes before starting again.
Once you’re done:
- Make sure the suction catheter and plastic tube are clean. Rinse and wipe the outside and suction water through the inside to clean them, if needed.
- Disconnect the suction catheter from the plastic tubing on the suction machine.
- Place the suction catheter on the dry cloth or paper towel.
- If you’re at home, empty the secretions from the inside of the suction machine into the toilet. Don’t empty them into the sink. They can clog the drain. In the hospital, a staff member will do this for you.
While you’re at home, change the suction catheter every week or more often if it’s dirty or clogged. While you’re in the hospital, you’ll use a new catheter each time you suction.
How to remove, clean, and reinsert your laryngectomy tube
Clean your laryngectomy tube regularly to help to keep it free of secretions. We recommend cleaning it at least twice a day or more often as needed. Your nurse will show you how.
-
Gather your supplies. You’ll need:
- A mirror
- A nylon tracheostomy brush
- Cotton neck tape
- Scissors
- Normal saline
- Cotton-tipped applicators
- Surgilube® (optional)
- A clean, dry cloth or paper towel (when you’re at home)
- Clean, dry gauze pads (when you’re in the hospital)
- Wash your hands well with soap and water.
- Stand or sit in front of a sink with a mirror.
- Untie or cut your neck tape.
- Remove the tube from your stoma.
-
Use the nylon brush to clean the inside of the laryngectomy tube (see Figure 5). Then hold the tube under warm running water.
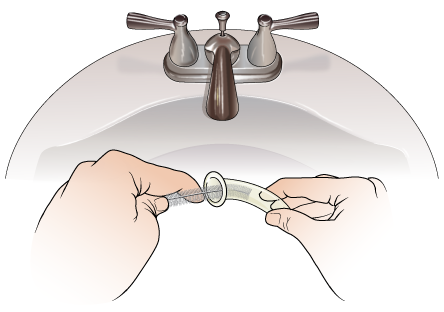
Figure 5. Cleaning your laryngectomy tube - Once the tube is clean, shake out the extra water. Dry the tube with a clean, dry cloth or paper towel. (If you’re in the hospital, use gauze instead.)
- Put clean neck tape in the slots on the side of the tube.
- Gently clean the skin around your stoma with normal saline using cotton-tipped applicators.
- Lubricate the outside of the tube with water or Surgilube.
- Tilt your chin slightly toward your chest.
-
Hold your breath and put the tube into your stoma (see Figure 6).
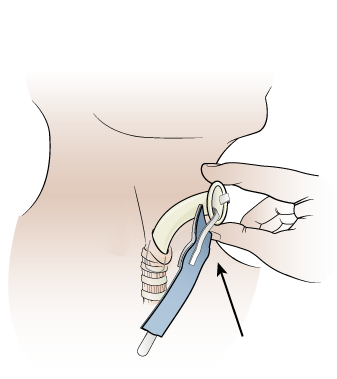
Figure 6. Inserting your laryngectomy tube - Tie the neck tape leaving 1 finger space between the tape and your neck.
- Rinse the nylon tracheostomy brush under running water.
Ways to communicate
You’ll need to learn a new way of speaking after your total laryngectomy. There are 3 options:
- An electrolarynx
- Esophageal speech
- Tracheoesophageal speech
All these options use an alternate sound source to make sound either outside your body using an electronic device or inside your body using the tissue and structures in your throat.
The type of surgery you had will determine which of these options you can use. Your speech therapist will explain these options before your surgery. After your surgery, they’ll monitor your progress to help you decide what options are right for you. All these communication options require practice and time.
Electrolarynx
An electrolarynx is a device you put against your neck to make your voice (see Figure 7). To speak, you use your mouth, lips, and tongue to shape the sound, like you did before your laryngectomy.
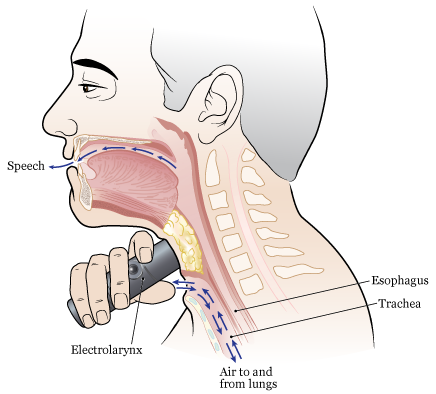
The new voice made with the electrolarynx won’t sound the same as your old one. It will sound more electronic. With practice, it can become more natural, with your own speech patterns and accents.
You can use an electrolarynx to speak as early as 3 to 5 days after your surgery. It’s easy to learn.
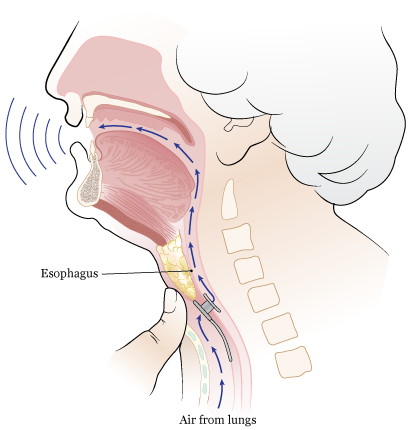
Esophageal speech
With esophageal speech, you make sounds by pushing or swallowing air into your esophagus, then pushing it back up through your throat and out of your mouth while shaping the sound of words with your mouth.
Esophageal speech sounds more natural than an electrolarynx, but it’s much harder to learn. It takes 3 to 6 months of training with a speech therapist.
Not everyone can learn esophageal speech. The extent of your surgery and your healing will determine if it’s an option for you.
Tracheoesophageal speech
With tracheoesophageal speech, your surgeon makes a hole between your trachea and esophagus using a procedure called a tracheoesophageal puncture (TEP). They can make the TEP during your laryngectomy surgery or as a separate procedure after you’ve healed. If it’s done as a separate procedure, it’s usually about 3 to 6 months after your total laryngectomy.
Something must always stay in your TEP tract or it will close, like a cut. Your surgeon will place either a thin catheter (tube) or a TEP prosthesis in your TEP tract to keep it open. A TEP prosthesis is a valve that lets you speak when it’s open and lets you eat and drink without aspiration (food or liquid entering your lungs) when it’s closed.
If your surgeon places a catheter in your TEP tract, your speech pathologist will replace it with a TEP prosthesis once the site has healed. This is usually about 10 to 12 days after the TEP is made.
To make tracheoesophageal speech, you must breathe in and then cover your stoma (see Figure 8). The air from your lungs will be forced through the TEP prosthesis and into your throat. Your throat will vibrate to make sound (see Figure 9). Tracheoesophageal speech sounds similar to your speech before your laryngectomy.

Emergency precautions for TEP
If you had a TEP, you’ll get a TEP Prosthesis Dislodgement Kit when you’re discharged from the hospital. This kit has written directions and different sized catheters in case your TEP prosthesis falls out. This isn’t likely to happen, but if it does, don’t panic. Follow the steps below.
- Get the 16FR width catheter from your TEP Prosthesis Dislodgement Kit. Knot it at the top.
-
Put the other end of the catheter into your TEP tract so 5 to 6 inches (13 to 15 centimeters) of the catheter is sticking out (see Figure 10). If you can’t get it in, try a thinner catheter.
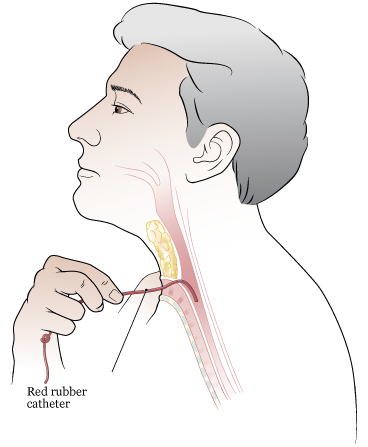
Figure 10. Inserting catheter into TEP tract -
Tape the knotted end to your chest or neck (see Figure 11). This will let you eat and drink until you can get to your speech therapist. They’ll put the TEP prosthesis back into your TEP tract.
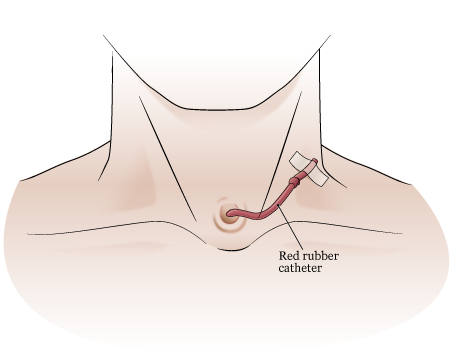
Figure 11. Taping catheter to neck - Call your speech therapist at MSK and tell them your TEP prosthesis fell out. If you can, find the prosthesis and bring it to your appointment.
If you can’t find the TEP prosthesis and think it may have fallen into your lungs:
- Put a catheter into your TEP tract following the steps above.
- Go to the Urgent Care Center at MSK. Ask for the Head and Neck doctor on call.
- If you aren’t near MSK, go to the nearest emergency room. Bring the TEP Prosthesis Dislodgement Kit with you and tell them there may be a foreign body in your lungs. They’ll need to do a chest x-ray and remove it if needed.
If you can’t put a catheter into your TEP tract:
- Don’t eat or drink anything.
- Between 9:00 a.m. and 5:00 p.m., call the Speech and Hearing Center at MSK at 212-639-5856 and tell them what happened.
- After 5:00 p.m., on weekends, and on holidays, go to the Urgent Care Center at MSK and ask for the Head and Neck doctor on call. If you aren’t near MSK, go to your nearest emergency department and tell them that you can’t insert a catheter into your TEP tract.
Physical activity and exercise
You can go back to doing most activities right after your surgery. Exercise will help you gain strength and feel better. Walking and stair climbing are excellent forms of exercise. Gradually increase the distance you walk. Climb stairs slowly, resting or stopping as needed. Ask your healthcare provider before starting more strenuous exercises.
Don’t lift anything heavier than 10 pounds (4.5 kilograms) for at least 2 weeks. Ask your healthcare provider how long to avoid heavy lifting.
Don’t go swimming or use hot tubs or saunas. It’s also best to avoid being on small boats because they have a higher chance of rolling over.
Driving
Ask your healthcare provider when you can drive. Most people can start driving again 3 weeks after surgery. Do not drive while you’re taking pain medicine that may make you drowsy.
You can ride in a car as a passenger at any time after you leave the hospital.
Going back to work
Talk with your healthcare provider about your job. They’ll tell you when it may be safe for you to start working again based on what you do. If you move around a lot or lift heavy objects, you may need to stay out a little longer. If you sit at a desk, you may be able to go back sooner.
Traveling
Having a tracheostomy or laryngectomy should not stop you from travelling. But check with your healthcare provider to talk about whether air travel is safe.
If you’re flying, contact your airline. Check if you need a letter from your healthcare provider for your medical equipment.
Place your medical equipment in your carry-on luggage in an area that’s easy to get to. Your medical equipment may include:
- Stoma care equipment (portable suction and catheters).
- An electrolarynx.
- TEP dislodge device.
You can manage cabin dry air by moistening the air. Wear a heat and moisture exchanger (HME) filter or a moist cloth cover over your stoma. HME filters include Provox XtraMoist HME and Provox Life Home HME.
Managing your feelings
You may have new and upsetting feelings after a surgery for a serious illness. Many people say they felt weepy, sad, worried, nervous, irritable, or angry at one time or another. You may find that you cannot control some of these feelings. If this happens, it’s a good idea to seek emotional support. Your healthcare provider can refer you to MSK’s Counseling Center. You can also reach them by calling 646-888-0200.
The first step in coping is to talk about how you feel. Family and friends can help. We can also reassure, support, and guide you. It’s always a good idea to let us know how you, your family, and your friends are feeling emotionally. Many resources are available to you and your family. We’re here to help you and your family and friends handle the emotional aspects of your illness. We can help no matter if you’re in the hospital or at home.
When to call your healthcare provider
Call your healthcare provider right away if:
- You have a fever of 100.5 °F (38 °C) or higher
- There’s drainage from your incision
- You have shortness of breath
- The skin around your incision is warmer than usual
- You have increased discomfort in the area around your incision
- The area around your incision is getting redder
- The area around your incision is starting to swell
- Swelling around your incision is getting worse
- Your stoma is blocked and affecting your breathing
- You have any questions or concerns
Contact information
Monday through Friday from to , contact your healthcare provider’s office.
After , during the weekend, and on holidays, call 212-639-2000 and ask to speak to the person on call for your healthcare provider.
Support services
This section has a list of support services. They may help you as you get ready for your surgery and recover after your surgery.
As you read this section, write down questions to ask your healthcare provider.
MSK support services
Admitting Office
212-639-7606
Call if you have questions about your hospital admission, such as asking for a private room.
Anesthesia
212-639-6840
Call if you have questions about anesthesia.
Blood Donor Room
212-639-7643
Call for information if you’re interested in donating blood or platelets.
Bobst International Center
www.msk.org/international
888-675-7722
We welcome patients from around the world and offer many services to help. If you’re an international patient, call for help arranging your care.
Counseling Center
www.msk.org/counseling
646-888-0200
Many people find that counseling helps them. Our Counseling Center offers counseling for individuals, couples, families, and groups. We can also prescribe medicine to help if you feel anxious or depressed. Ask a member of your care team for a referral or call the number above to make an appointment.
Food Pantry Program
646-888-8055
We give food to people in need during their cancer treatment. Talk with a member of your care team or call the number above to learn more.
Integrative Medicine and Wellness Service
www.msk.org/integrativemedicine
Our Integrative Medicine and Wellness Service offers many services to complement (go along with) traditional medical care. For example, we offer music therapy, mind/body therapies, dance and movement therapy, yoga, and touch therapy. Call 646-449-1010 to make an appointment for these services.
You can also schedule a consultation with a healthcare provider in the Integrative Medicine and Wellness Service. They’ll work with you to make a plan for creating a healthy lifestyle and managing side effects. Call 646-608-8550 to make an appointment for a consultation.
MSK Library
library.mskcc.org
You can visit our library website or email [email protected] to talk with the library reference staff. They can help you find more information about a type of cancer. You can also visit the library’s Patient Education Resource Guide.
Nutrition Services
www.msk.org/nutrition
212-639-7312
Our Nutrition Service offers nutritional counseling with one of our clinical dietitian nutritionists. Your clinical dietitian nutritionist will talk with you about your eating habits. They can also give advice on what to eat during and after treatment. Ask a member of your care team for a referral or call the number above to make an appointment.
Patient and Community Education
www.msk.org/pe
Visit our patient and community education website to search for educational resources, videos, and online programs.
Patient Billing
646-227-3378
Call if you have questions about preauthorization with your insurance company. This is also called preapproval.
Patient Representative Office
212-639-7202
Call if you have questions about the Health Care Proxy form or concerns about your care.
Perioperative Nurse Liaison
212-639-5935
Call if you have questions about MSK releasing any information while you’re having surgery.
Private Duty Nurses and Companions
646-357-9272
You can request private nurses or companions to care for you in the hospital and at home. Call to learn more.
Rehabilitation Services
www.msk.org/rehabilitation
Cancers and cancer treatments can make your body feel weak, stiff, or tight. Some can cause lymphedema (swelling). Our physiatrists (rehabilitation medicine doctors), occupational therapists (OTs), and physical therapists (PTs) can help you get back to your usual activities.
- Rehabilitation medicine doctors diagnose and treat problems that affect how you move and do activities. They can design and help coordinate your rehabilitation therapy program, either at MSK or somewhere closer to home. Call Rehabilitation Medicine (Physiatry) at 646-888-1929 to learn more.
- An OT can help if you’re having trouble doing usual daily activities. For example, they can recommend tools to help make daily tasks easier. A PT can teach you exercises to help build strength and flexibility. Call Rehabilitation Therapy at 646-888-1900 to learn more.
Resources for Life After Cancer (RLAC) Program
646-888-8106
At MSK, care does not end after your treatment. The RLAC Program is for patients and their families who have finished treatment.
This program has many services. We offer seminars, workshops, support groups, and counseling on life after treatment. We can also help with insurance and employment issues.
Sexual Health Programs
Cancer and cancer treatments can affect your sexual health, fertility, or both. MSK’s sexual health programs can help you before, during, or after your treatment.
- Our Female Sexual Medicine and Women’s Health Program can help with sexual health problems such as premature menopause or fertility issues. Ask a member of your MSK care team for a referral or call 646-888-5076 to learn more.
- Our Male Sexual and Reproductive Medicine Program can help with sexual health problems such as erectile dysfunction (ED). Ask a member of your care team for a referral or call 646-888-6024 to learn more.
Social Work
www.msk.org/socialwork
212-639-7020
Social workers help patients, families, and friends deal with common issues for people who have cancer. They provide individual counseling and support groups throughout your treatment. They can help you communicate with children and other family members.
Our social workers can also help refer you to community agencies and programs. If you’re having trouble paying your bills, they also have information about financial resources. Call the number above to learn more.
Spiritual Care
212-639-5982
Our chaplains (spiritual counselors) are available to listen, help support family members, and pray. They can contact community clergy or faith groups, or simply be a comforting companion and a spiritual presence. Anyone can ask for spiritual support. You do not have to have a religious affiliation (connection to a religion).
MSK’s interfaith chapel is located near Memorial Hospital’s main lobby. It’s open 24 hours a day. If you have an emergency, call 212-639-2000. Ask for the chaplain on call.
Tobacco Treatment Program
www.msk.org/tobacco
212-610-0507
If you want to quit smoking, MSK has specialists who can help. Call to learn more.
Virtual Programs
www.msk.org/vp
We offer online education and support for patients and caregivers. These are live sessions where you can talk or just listen. You can learn about your diagnosis, what to expect during treatment, and how to prepare for your cancer care.
Sessions are private, free, and led by experts. Visit our website to learn more about Virtual Programs or to register.
External support services
Access-A-Ride
web.mta.info/nyct/paratran/guide.htm
877-337-2017
In New York City, the MTA offers a shared ride, door-to-door service for people with disabilities who can’t take the public bus or subway.
Air Charity Network
www.aircharitynetwork.org
877-621-7177
Provides travel to treatment centers.
American Cancer Society (ACS)
www.cancer.org
800-ACS-2345 (800-227-2345)
Offers a variety of information and services, including Hope Lodge, a free place for patients and caregivers to stay during cancer treatment.
Cancer and Careers
www.cancerandcareers.org
646-929-8032
A resource for education, tools, and events for employees with cancer.
CancerCare
www.cancercare.org
800-813-4673
275 Seventh Avenue (Between West 25th & 26th Streets)
New York, NY 10001
Provides counseling, support groups, educational workshops, publications, and financial assistance.
Cancer Support Community
www.cancersupportcommunity.org
Provides support and education to people affected by cancer.
Caregiver Action Network
www.caregiveraction.org
800-896-3650
Provides education and support for people who care for loved ones with a chronic illness or disability.
Corporate Angel Network
www.corpangelnetwork.org
866-328-1313
Offers free travel to treatment across the country using empty seats on corporate jets.
Good Days
www.mygooddays.org
877-968-7233
Offers financial assistance to pay for copayments during treatment. Patients must have medical insurance, meet the income criteria, and be prescribed medicine that’s part of the Good Days formulary.
HealthWell Foundation
www.healthwellfoundation.org
800-675-8416
Provides financial assistance to cover copayments, health care premiums, and deductibles for certain medicines and therapies.
Joe’s House
www.joeshouse.org
877-563-7468
Provides a list of places to stay near treatment centers for people with cancer and their families.
LGBT Cancer Project
www.lgbtcancer.com
Provides support and advocacy for the LGBT community, including online support groups and a database of LGBT-friendly clinical trials.
LIVESTRONG Fertility
www.livestrong.org/fertility
855-744-7777
Provides reproductive information and support to cancer patients and survivors whose medical treatments have risks associated with infertility.
Look Good Feel Better Program
www.lookgoodfeelbetter.org
800-395-LOOK (800-395-5665)
This program offers workshops to learn things you can do to help you feel better about your appearance. For more information or to sign up for a workshop, call the number above or visit the program’s website.
National Cancer Institute
www.cancer.gov
800-4-CANCER (800-422-6237)
National Council on Aging (NCOA)
www.benefitscheckup.org
Provides information and resources for older adults. Offers BenefitsCheckUp®, a free online tool that connects you to prescription assistance programs, including Medicare’s Extra Help program.
National LGBT Cancer Network
www.cancer-network.org
Provides education, training, and advocacy for LGBT cancer survivors and those at risk.
Needy Meds
www.needymeds.org
Lists Patient Assistance Programs for brand and generic name medicines.
NYRx
www.health.ny.gov/health_care/medicaid/program/pharmacy.htm
Provides prescription benefits to eligible employees and retirees of public sector employers in New York State.
Patient Access Network (PAN) Foundation
www.panfoundation.org
866-316-7263
Gives help with copayments for patients with insurance.
Patient Advocate Foundation
www.patientadvocate.org
800-532-5274
Provides access to care, financial assistance, insurance assistance, job retention assistance, and access to the national underinsured resource directory.
Red Door Community (formerly known as Gilda’s Club)
www.reddoorcommunity.org
212-647-9700
A place where people living with cancer find social and emotional support through networking, workshops, lectures, and social activities.
RxHope
www.rxhope.com
877-267-0517
Provides assistance to help people get medicines they have trouble affording.
Triage Cancer
www.triagecancer.org
Provides legal, medical, and financial information and resources for cancer patients and their caregivers.
Laryngectomy, oral cancer, and head and neck cancer support services
Support for People with Oral and Head and Neck Cancer (SPOHNC)
www.spohnc.org
800-377-0928
Provides information and support for people with oral and head and neck cancer.
Web Whispers
www.webwhispers.org
Provides information and support for people who had laryngectomies and survivors of laryngeal cancer.
Educational resources
This section lists the educational resources mentioned in this guide. They will help you get ready for your surgery and recover after your surgery.
As you read these resources, write down questions to ask your healthcare provider.
- A Guide for Caregivers
- Common Questions About MSK's Recovery Tracker
- Advance Care Planning for People With Cancer and Their Loved Ones
- How To Check if a Medicine or Supplement Has Aspirin, Other NSAIDs, Vitamin E, or Fish Oil
- Herbal Remedies and Cancer Treatment
- How to Be a Health Care Agent
- Patient-Controlled Analgesia (PCA)
Learn about our Health Information Policy.
